
Knee pain on the bike: why the knee is rarely the problem
Knee pain is one of the most common reasons cyclists seek help. And also one of the most misunderstood.Patellofemoral pain. IT band irritation. Medial knee pain. Pain behind the knee. Pain that appears only after 40 minutes. Pain that disappears when you stop riding and comes back the next ride.
Many riders are told the same thing:
“Your knee is overloaded.”
“Your muscles are weak.”
“Rest more.”
“Strengthen your quads.”
And yet, the problem persists.
In our experience, most cycling-related knee problems do not originate in the knee itself.
The knee is rarely the cause. It is far more often the endpoint of a much larger system that is out of balance.
The Knee: a follower, not a leader
Biomechanically, the knee is a relatively simple joint.
It flexes and extends. It tolerates very little rotation. It depends heavily on what happens above and below it.
The knee does not decide how you move. It follows instructions.
Those instructions come from:
the foot and ankle
the hip and pelvis
the spine
and, crucially, the nervous system
When something in that chain is off structurally, motorically, or neurologically, the knee absorbs the consequences.
Different knee pain, same story
Over the years, we’ve worked with hundreds of cyclists suffering from different types of knee pain. While the location of the pain differs, the underlying mechanisms often overlap.
Patellofemoral pain
Pain around or behind the kneecap is frequently linked to:
altered hip control
pelvic instability
excessive femoral internal or external rotation
motor timing issues rather than strength deficits
The kneecap tracks differently not because the knee is “bad”, but because the system guiding it is inconsistent.
IT band–related pain
ITB complaints are rarely an isolated tissue problem.
They are often the result of:
asymmetrical pelvic control
excessive lateral compensation
one side doing more stabilisation work than the other
The IT band becomes a secondary stabiliser when the primary ones fail.
Medial knee pain
Often associated with:
stance width issues (Q-factor)
foot rotation and cleat position
motor strategies that force the knee inward under load
The knee is forced into positions it was never designed to tolerate repetitively.
Pain behind the knee
Commonly linked to:
overactive hamstrings
dead spots in the pedal stroke
compensation for lack of proximal drive
Again, the knee pays the price for what the system fails to organise upstream.
The missing layer: motor control and preference
This is where most bikefitting stops, and where we deliberately go further.
Humans are not symmetrical machines. The brain always has a preferred side. A preferred strategy. A preferred way of organising movement. Two legs can produce identical power numbers while being motorically completely different.
One leg may:
initiate movement faster
stabilise better
tolerate load more easily
The other may:
arrive late
compensate
search for stability
Power meters rarely show this. But the body always does. Knee pain often appears when the nervous system is forced into a position it does not trust, and compensates through the knee.
Why “perfect positioning” often fails
A position can look perfect on paper:
ideal knee angles (measured with Retül, Idmatch, Velogicfit, other softwares)
symmetrical saddle height
neutral cleat alignment
And still cause pain.
Why?
Because a mechanically correct position can be neurologically expensive.
If the brain has to work too hard to maintain stability, the body will offload that effort somewhere.
Very often, that “somewhere” is the knee.
How we actually analyse knee problems
We don’t guess. We measure, across multiple layers.
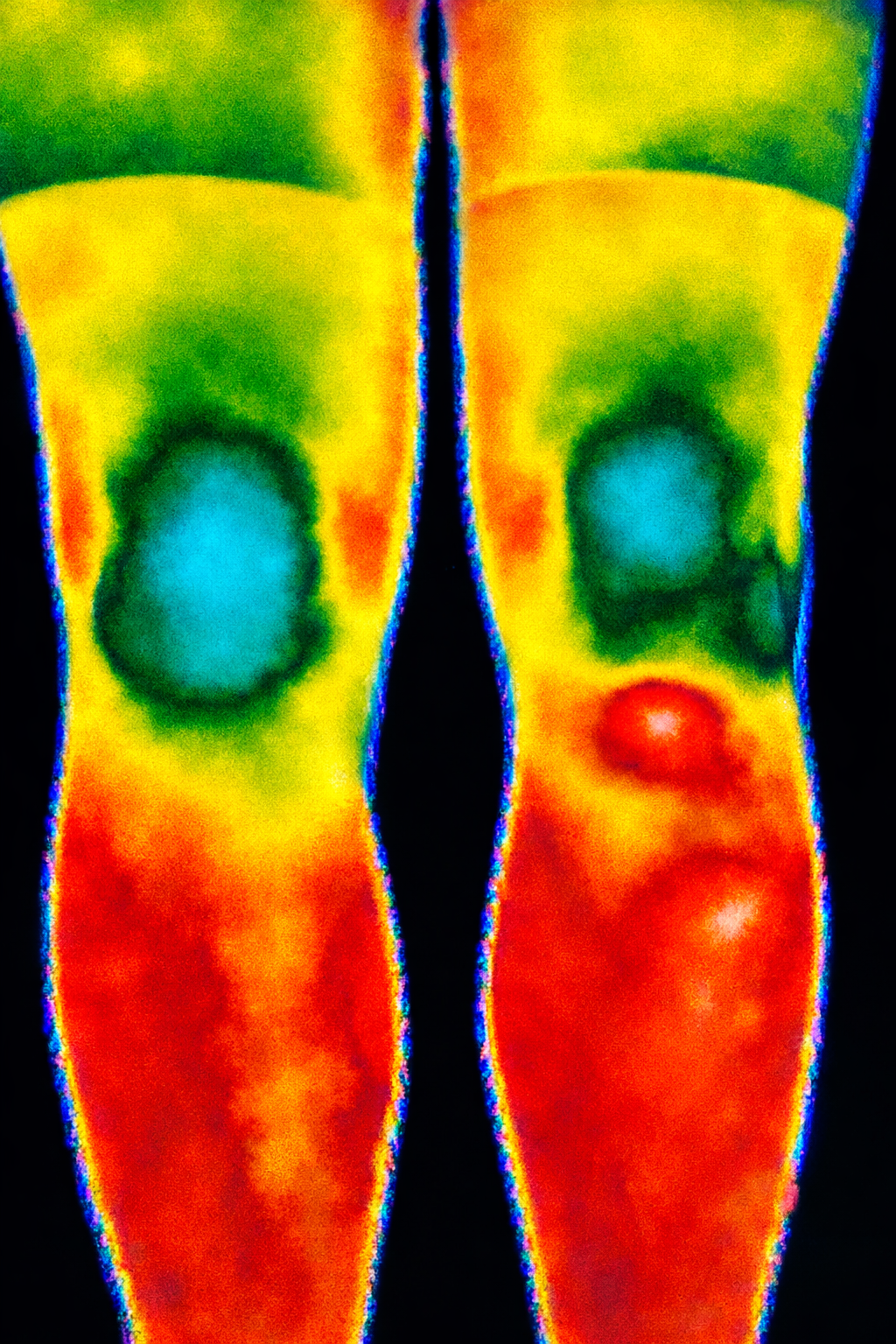
Thermal imaging
We use thermal cameras to detect:
asymmetrical load patterns
areas of chronic overuse
regions of reduced activation or inhibition
Heat rarely lies.
EMG measurements
Electromyography allows us to see:which muscles are working too much
which muscles are underperforming
timing differences between left and right
This is where “weakness” often turns out to be a motor control issue, not a strength one.
Motor control testing
Simple, targeted tests off the bike reveal:
delayed reactions
side dominance
reduced automatic control
These patterns almost always reappear on the bike.
Spine and pelvic scanning
We analyse:
pelvic orientation
spinal torsion
weight distribution
Knee pain is often a downstream effect of subtle axial asymmetries.
Leg length and structural assessment
True structural differences matter.
But functional asymmetry matters more.
Correcting the wrong thing can worsen the problem.
In-house motion sensors
We use proprietary data tools to:
track stability over time
detect dead spots in the pedal stroke
measure how changes affect the system, not just the joint
This allows us to see whether an intervention actually reduces the body’s need to compensate.
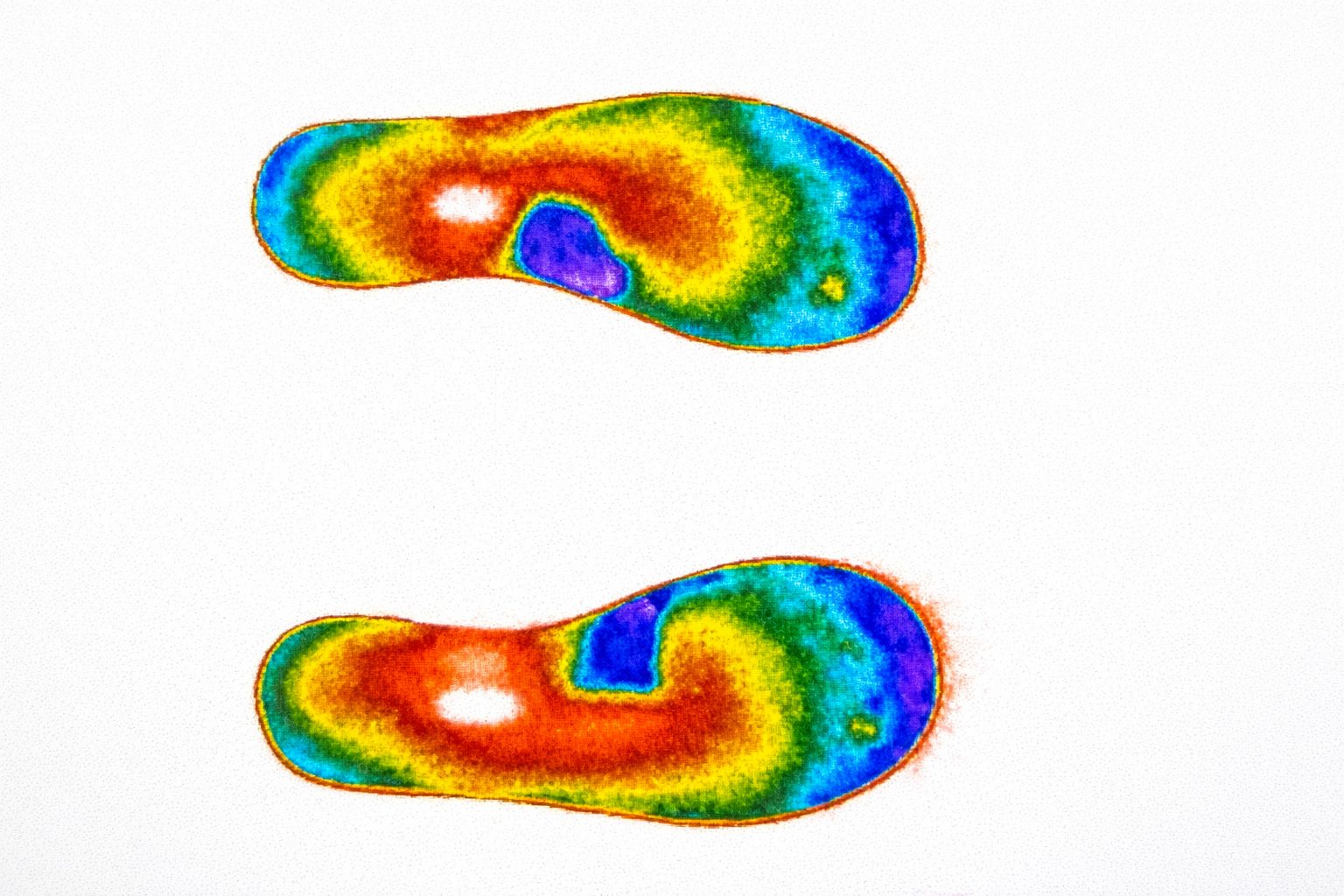
Cleats: small component, huge consequences
Cleat position is often treated as a technical detail.
In reality, it is a neurological interface.
Cleat fore–aft, rotation and stance width can:
support or fight a rider’s motor strategy
increase or decrease knee load dramatically
change how the brain organises force production
Sometimes moving a cleat forward creates more stability.
Sometimes moving it back creates more control.
There is no universal rule, only individual motor logic.
Why many cyclists feel “out of options”
We see many riders who have already:
visited multiple physiotherapists
seen osteopaths
received injections
been told to rest
And still hurt. Not because those approaches are wrong, but because the core driver was never addressed. The bike position did not match how the rider’s body and brain actually work.
Final thought
If you have knee pain on the bike, the most important question is not:
“What’s wrong with my knee?”
It’s:
“What is my body compensating for?”
That’s where real answers begin. And that’s where our work starts.